A University of Colorado team evaluated the reliability of the Richmond Agitation-Sedation Scale in mechanically ventilated patients in the intensive care unit.
Read the source article for this feature from Critical Care Explorations.
A University of Colorado team evaluated the reliability of the Richmond Agitation-Sedation Scale (RASS) in mechanically ventilated patients in the intensive care unit (ICU). Their findings were published in the September 2025 issue of
Critical Care Explorations.
1
The RASS is a 10-level scale that ranges from −5 (unarousable) to 0 (alert and calm) to +4 (combative).
2 Introduced in 2002, the RASS has become the standard bedside tool for assessing sedation and agitation in adult patients in the ICU.
2
The Society of Critical Care Medicine’s 2018 pain, agitation/sedation, delirium, immobility, and sleep disruption (PADIS) guidelines recommend light sedation for critically ill mechanically ventilated adults.
3 Light sedation is associated with shorter time to extubation and reduced tracheostomy rate, although there is no consensus on the definitions of light, moderate, and deep sedation.
3
First author Mikita Fuchita, MD, is an intensivist and anesthesiologist at University of Colorado Hospital and assistant professor of anesthesiology at University of Colorado Anschutz. He became interested in how RASS performed in his ICU and whether clinicians rating a patient at the same time agreed on the score. “Sedation management practices vary from place to place,” Dr. Fuchita said. “However, most ICUs around the country default to a deep sedation approach for patients with an oral endotracheal tube.”
4,5
Dr. Fuchita’s cardiothoracic ICU team were struggling to implement a minimal sedation approach for mechanically ventilated adults, as the PADIS guidelines recommend. He was also concerned about the mental health effects of sedation on mechanically ventilated patients, who often receive a continuous infusion of sedatives to spare them the discomfort and fear of mechanical ventilation. But studies have shown that deep sedation does not improve patients’ psychological well-being and that memories of events occurring during critical illness—even unpleasant ones—may protect against anxiety and future posttraumatic stress disorder.
6,7 Some patients have reported that sedation itself was a traumatizing experience.
8
In 2022, the team launched a quality improvement initiative designed to change their approach to sedation management. “We’re really trying to build a culture where all the interdisciplinary ICU professionals have an aligned vision that, whenever possible, we should be trying to minimize sedation and achieve a RASS score of 0,” Dr. Fuchita said.
The Findings
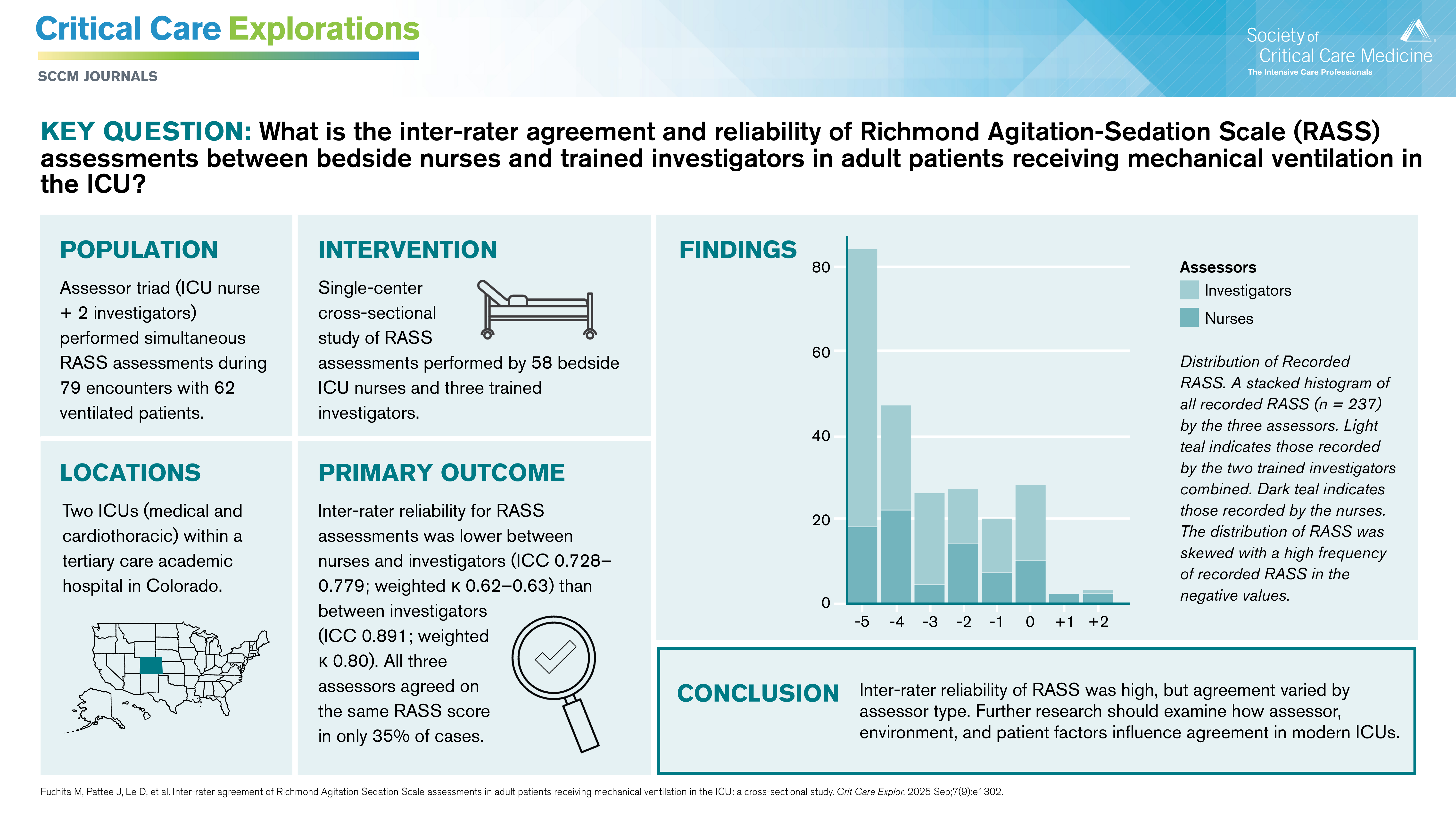
To evaluate the RASS’s inter-rater reliability, the team compared the assessments of a triad of RASS assessors: two trained investigators and a bedside ICU nurse. In total, three trained investigators and 58 nurses participated in the study.
RASS assessments were performed a median of 3.5 days after initiation of mechanical ventilation. Because RASS scores can vary throughout the day, the triad independently rated each patient at the same time. They rated 79 encounters with 62 unique patients receiving mechanical ventilation in the University of Colorado Hospital medical ICU and cardiothoracic ICU. If assessors felt uncertain about a score, the team asked them to submit comments.
The three assessors in each triad agreed on RASS score in only 35% of observations. The differences were mostly small, a difference of one sedation level or less. The average differences in RASS scores were greater between the trained investigators and nurses, ranging from –0.658 to –0.544, compared with 0.114 between the two trained investigators.
Nurses recorded higher RASS scores (lighter sedation level) in 52% of observations. Most patients (72%) had a target RASS score of –1 to +1. The most common RASS score (35%) was –5, the deepest sedation level.
These findings confirmed Dr. Fuchita’s concern that some patients may be receiving deeper sedation than necessary. Yet, maintaining a lighter sedation level throughout the day can be challenging for patients on continuous sedation infusions. Nurses have expressed concerns about patients on lighter sedation becoming restless or agitated, which can lead to self-extubation or accidental extubation.
ICU clinicians often face the challenging task of personalizing sedation for each patient, such as those with severe acute respiratory distress syndrome. “Whenever you lighten sedation, oxygenation may drop or there may be a ventilator dyssynchrony,” Dr. Fuchita said. “There’s a competing interest between sedation and ventilator management. Large tidal volumes are known to be harmful for the patient, but deep sedation is also harmful. So what’s the right balance?”
In 16% of the study observations, at least one assessor submitted comments indicating uncertainty. Some ambiguity resulted from interpretation of eye opening and two levels of stimulation, verbal and physical, Dr. Fuchita said. Patients with some conditions cannot move or open their eyes even when they are awake and cognitively intact. “The RASS really relies on how long patients can maintain eye opening and eye contact, so those patients become very challenging to reliably assess,” he said. “The RASS doesn’t really provide what to do in those specific contexts.”
What’s Next
The study confirmed the reliability of using the RASS at the bedside, although scores varied slightly by assessor. “Our result was reassuring that overall reliability of the scale is good, so it gave us some level of confidence that we can continue using this to track our trend in our sedation practices,” Dr. Fuchita said.
Further research could explore factors influencing the differences between assessors or could evaluate other objective ways to assess sedation, such as accelerometry, EEG, or video recording. “But when you think about real-world implementation, it needs to be feasible, implementable, and scalable. I think this affirms that, for now, we should stick with the RASS as a reliable tool.”