Evidence-based clinical guidelines are a mainstay of medicine, yet they are difficult to implement in critical care. The authors of a recent study developed and tested a software system that successfully evaluated guideline adherence across multiple hospital systems and IT software.
Read the source article for this feature from Critical Care Medicine.
Evidence-based clinical guidelines are a mainstay of medicine, yet they are difficult to implement in critical care. The complexity of treating critically ill and injured patients makes it a constant challenge for clinicians to track and apply every relevant guideline in real time, according to Falk von Dincklage, MD, deputy director of the Department of Anesthesia, Critical Care, Emergency, and Pain Medicine at Greifswald University Hospital in Greifswald, Germany.
“Critical care clinicians are expected to stay current not only on their own specialty’s guidelines but also on every specialty relevant to their patients—and apply them flawlessly in real time,” Dr. von Dincklage said. “This is where a computer system might take off a bit of the load.”
To improve the real-world use of clinical guidelines in critical care medicine—and ultimately improve patient care and safety—Dr. von Dincklage has partnered on several projects with Gregor Lichtner, PhD, a medical data scientist in the same department at Greifswald University Hospital. For their latest collaboration, they developed and tested a software system that successfully evaluated guideline adherence across multiple hospital systems and IT software.
This new automated system can provide real-time decision support and, unlike hard-coded guideline software, can incorporate updated clinical guidelines without requiring changes to the software. The new system could enhance large-scale decision support, informing targeted interventions and improving patient care, Dr. von Dincklage said. Their findings were published in the January 2026 issue of
Critical Care Medicine.
1
The Findings
Current automated guidelines systems require that recommendations be rewritten in a way that computers can interpret. Previously proposed formats were often developed for a specific institution’s technical environment and are therefore difficult to use across hospitals with different IT environments. To address this problem, the research team previously developed a digital guideline format based on the modern interoperability standard Fast Healthcare Interoperability Resources (FHIR).
2
Recognizing the wide variability in how each hospital stores patient data, the team recently expanded its FHIR-based model to be used with the Observational Medical Outcomes Partnership Common Data Model, a standardized framework for representing clinical data.
3
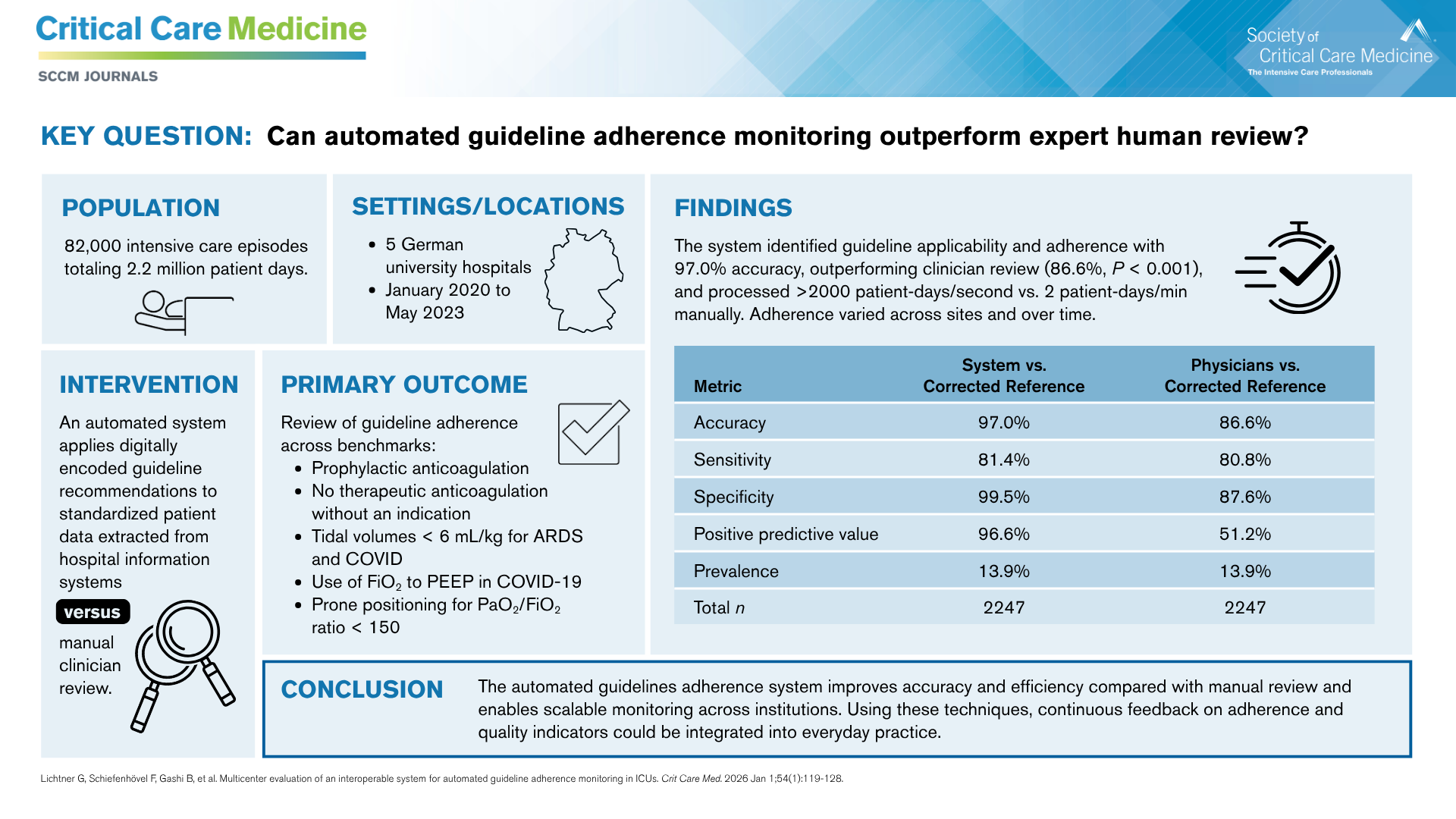
The team tested its new system in a retrospective observational study that evaluated guideline adherence at five university hospitals in Germany, examining data from 82,000 intensive care episodes from January 2020 to May 2023.
1 To demonstrate the system’s adaptability to rapidly evolving guidelines, the team selected six representative recommendations, focused primarily around COVID-19-related treatments, from a set of 41 critical care guidelines.
For each patient and recommendation, the system determined whether the recommendation was applied and whether it was followed. Manual clinician reviews were conducted by seven intensive care physicians in three hospitals to validate the system’s interpretation of the recommendations. The reviewers were otherwise uninvolved in the study and unaware of the system implementation.
The system achieved 97% accuracy in identifying guideline applicability and adherence, compared with 86.6% accuracy by clinician manual review. Clinician review required 150 hours, or about 30 seconds per patient, while the system evaluated more than 2000 patient days per second on a standard computer. Clinician reviewers misclassified 296 (13.2%) cases that the system got right, while the system misclassified 63 (2.8%) cases that clinician reviewers got right.
Clinicians’ most common errors were due to oversight, particularly with large volumes of ventilation data. Other errors were caused by difficulties in interpreting loosely worded guidelines. For example, a tidal volume recommendation did not provide the formula for calculating predicted body weight, and clinicians use different formulas. Similarly, drug-related recommendations did not always define contraindications, which left room for interpretation.
The system errors were almost all related to lack of consideration of data, often because diagnoses were recorded in free-text fields.
What’s Next
The findings show that the guideline adherence monitoring approach can be integrated into diverse hospital IT environments despite variability in local software systems, with automatic updating of guideline logic when guideline revisions are published. Smaller and community hospitals that lack specialists who are knowledgeable about many different guidelines would particularly benefit, Dr. von Dincklage said.
Guideline development should consider real-word hospital IT environments in addition to clinical application, Dr. Lichtner said. “One thing that would be beneficial during the guideline development process is for the guideline panel to co-develop machine-readable versions of the recommendations. IT professionals and clinicians would work side by side to develop the guidelines to make the recommendations more actionable and more precise.”
Including IT professionals in guideline development would also help uncover ambiguous recommendations, which healthcare professionals steeped in the guidelines might not notice, Dr. von Dincklage said. “When we include technicians in the process of formulating machine-readable guideline versions, we as clinicians discover we were ambiguous.” When a technician asks clinicians to clarify what they meant in a particular recommendation, the clinicians may realize half of them meant one thing while the other half meant another.
“The difference with a clinical decision support system like this one is that we have rules that are curated, which are checked by experts, who are actually reliable and trustworthy,” Dr. von Dincklage said. “So we believe that rule-based systems, in comparison to many AI-based systems, have a higher chance of gaining clinicians’ trust and actually being used by clinicians.”